healthcare
Application-centric and data-centric interoperability
By
Tomaž Gornik
Healthcare is undergoing a transformation to an integrated, multi-provider model where the patient or more appropriately the citizen sits firmly at the centre. The focus has clearly shifted from individual care episodes to continuity of care and finally to holistic, population health management. It is not individual providers but governments at municipal, regional or national level that are starting to coordinate health and social care to help manage a citizen’s wellbeing.
This change in focus has many implications for IT systems, an area where healthcare providers already struggle. Clearly, the systems of today need to change since IT is a key enabler of this shift and interoperability is at the core of this challenge.
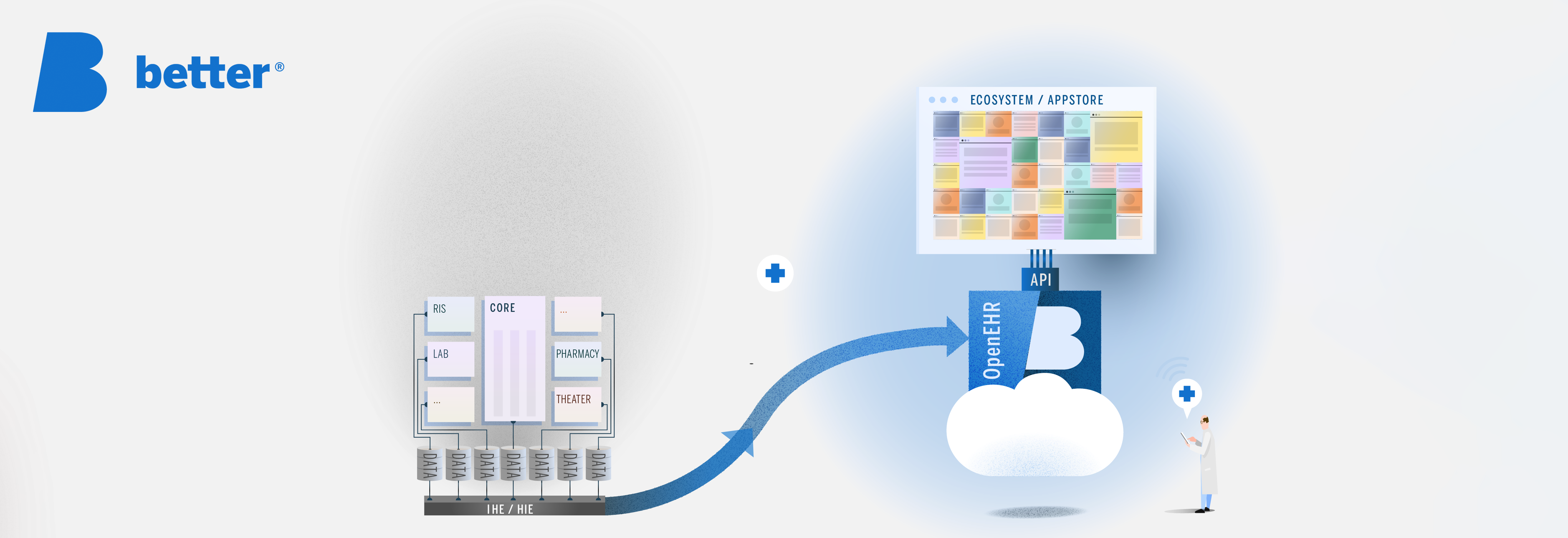
When it comes to health data interoperability, there are two schools of thought: application-centric and data-centric. The first believes that since there are so many systems already in place, we should agree on the exchange format (and recently the APIs) and convert the proprietary data into that format as needed. This is the preferred approach today when faced with a large installed base of legacy solutions. The focus here is on the applications.
The second approach is normalising the health data first, building new systems on top and avoiding the interoperability issues altogether. This entails defining a data layer, which is the most important aspect of an open architecture. Why is this the most important layer? Most healthcare organisations are beginning to realise that their data is more valuable than their applications. Data has become a valuable asset, since good data is key to improving outcomes, managing chronic disease and enabling population health management.
The focus shifts from applications to data, i.e. the data-centric approach.
To do this, storing the data in a vendor-neutral format is crucial. Almost all applications store data in proprietary formats and healthcare is no exception. What is different in healthcare is that we need to keep data for the lifetime of the patient. It is clear that no application will last this long so we will be migrating data from one proprietary format to another every 10 to 15 years when replacing applications. PACS is a good example. The DICOM format was chosen 30 years ago and today, no vendor stores images in other formats. But unlike images, structured clinical data is still being kept in the silos of the applications that produced it making data unavailable to others.
While this problem has been well known for decades, it is now centre stage driven by the transformation of healthcare. A year ago, Gartner Group published a research paper named “A Roadmap for a Citizen-Centric Integrated Model of Care” (login required) where they clearly state: “Gartner believes that truly effective and sustainable open architectures will need a capability for vendor-neutral data persistence, such as utilizing a common schema or set of archetypes and rules for managing structured and unstructured data (for example, a VNA, openEHR or IHE XDS repository in combination with services for trust/consent, ecosystem governance and oversight, and reuse of data and processes for secondary purposes, such as research and population health). Providing open messaging standards (for example, FHIR, HL7) for data exchange in specific use cases will only go so far in meeting the architectural challenges of digital citizen-centric care delivery.”[1]
So how do we get from an application-centric view to a data-centric one? Let’s take a look at the three steps:
1. Integrate
Most healthcare providers have many, many applications. When the GDPR directive came into force last year and providers had to catalogue their systems, larger trusts discovered they had hundreds of applications. All of them have patient data. All in a vendor’s proprietary format.
In order to make the best use of it, data needs to be extracted to build a lifetime health record describing the health status of the patient as accurately as possible. Using integration engines, data dumps, messaging or APIs, data is collected from as many applications as possible. Of course, this is a process and will not happen overnight. The first step is to focus on one or two areas where you are looking to innovate by buying or building a new app or application.
2. Open
Once you have access to this data, normalise it to a vendor-neutral format and cross map different coding to standard terminologies. This means using standards like openEHR for structured data, IHE XDS for documents and DICOM for imaging as Gartner suggests.
Other sources, like the NHS Apperta “Defining an open platform” whitepaper state: “openEHR is the only currently available open standard for the representation of fine-grained structured clinical content that is sufficiently mature and proven at scale.” Also “IHE-XDS and openEHR work well together, and this combination has been used successfully at scale. XDS handles unstructured and semi-structured data while openEHR handles fine-grained structured data with links between the openEHR clinical data repository and the XDS VNA enabling the creation of a seamless record.”
3. Innovate
It’s now time to take advantage of this consistent, longitudinal record to enable innovation.
How do we do innovation today? – we build a feral system! On the positive side, because they are driven by end-users, feral systems fill many gaps, are developed quickly, solve real problems and can also be very innovative. They often become essential for users to carry out their daily work. But there is another side to feral systems. For one, lack of integration with core systems prevents the sharing of data, requiring users to enter the same data repeatedly. Think about GDPR compliance and lack of governance. While innovative, feral systems are often not built or managed properly and thus pose serious risks to organisations.
What if you could buy or build new, innovative apps and put them on top of consistent data? Think patient engagement, precision medicine, clinical decision support, pathways and guidelines and how much easier it would be to build these solutions on a common data layer using predictive analytics, algorithms, machine learning and AI! You could now build an ecosystem of apps and applications which share data without additional integration. As long as apps commit to accessing and storing all data in this patient record, you can grow the ecosystem, taking advantage of innovation from different vendors. This architecture is fuelling the next generation of solutions known as the Postmodern EHR.
Conclusion
As mentioned above, most healthcare IT today is application-centric. To unleash innovation, IT has to start moving from the current state to a data-centric world. This requires three fundamental steps: integrate, open, innovate: use interoperability standards to integrate existing systems and data. Storing data in an open, vendor-neutral format will then enable ecosystems of vendors to innovate.
To see evidence of success with this approach, we need to look at the early adopters: countries like Slovenia and Norway, cities like Moscow, trusts like Plymouth, Taunton, Salford Royal and South London and Maudsley.
Remember: Integrate. Open. Innovate!
This article was published as part of the Interoperability – Advisory Series on digitalhealth.net
1: Mike Jones: Healthcare Provider CIOs Need to Rally Their Enterprise Architects Around Citizen-Centric Care Delivery. Gartner Group. Accessible at: https://www.gartner.com/document/3597430 (login required)
Read also: